KKR loaded America’s biggest ER staffing company with $8 billion in debt. When the math broke, the patients did not stop showing up. Harvard counted the deaths.
When private equity firm KKR acquired Envision Healthcare in October 2018 for $9.9 billion [1], loading the company with $8 billion in new debt [1], it was betting that a captive patient population, mandatory federal treatment requirements, and aggressive out-of-network billing would generate sufficient returns to service that debt. The bet failed. The patients did not walk away. On May 15, 2023, Envision filed for Chapter 11 bankruptcy [2], listing $7 billion in liabilities [2]. What the company left behind was not just a financial wreckage, it was a documented pattern of understaffing, clinical pressure, and preventable patient harm that Harvard researchers would eventually link to a measurable rise in emergency room deaths.
This is the story of how American emergency medicine was systematically acquired, exploited, and extracted for private profit, and what happens when the math doesn’t work out but the patients still show up.
The Official Story
Private equity firms argue that professional management, capital investment, and operational scale make healthcare systems more efficient. The pitch to hospital administrators is straightforward: outsourcing your emergency department physicians to a staffing company eliminates the administrative burden of physician employment, provides access to a national physician network, and allows hospitals to focus on their core operations. For patients, the industry claims, this translates to consistent quality of care regardless of location. For the broader healthcare system, the argument goes, capital investment enables technology upgrades and infrastructure improvements that cash-strapped hospitals couldn’t otherwise afford.
The data accumulated since 2018 does not support this argument as applied to emergency medicine [3][4].
Follow the Money
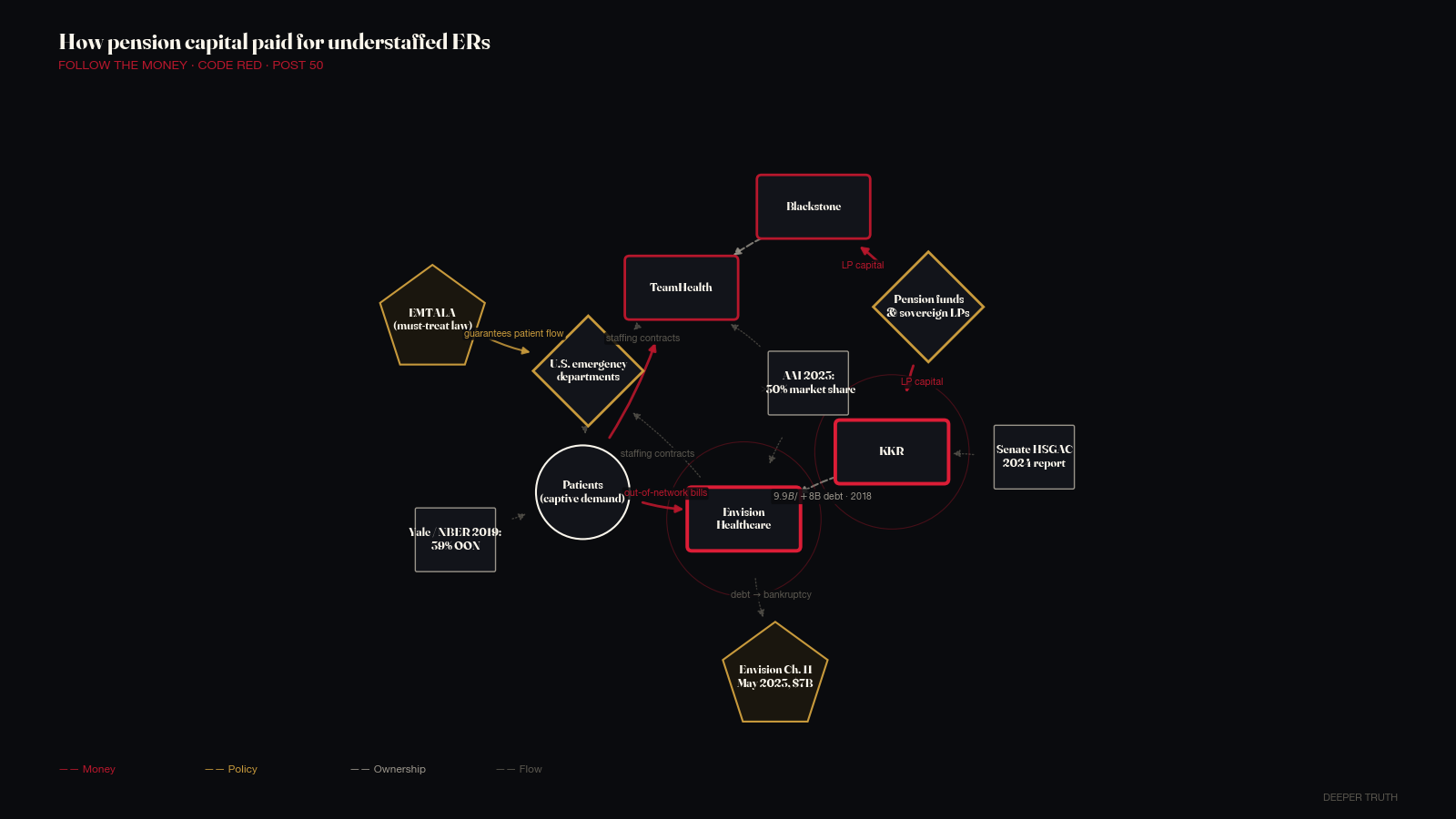
The private equity model in emergency medicine follows a specific financial logic. Emergency departments operate under the Emergency Medical Treatment and Active Labor Act, which requires hospitals to treat any patient who presents, regardless of ability to pay. That guarantees patient volume. You cannot opt out of an emergency. Private equity firms identified ER physician staffing as a captive revenue stream, and acquired the companies that staffed those departments.
The two dominant players were Envision Healthcare, backed by KKR, and TeamHealth, backed by Blackstone. Together they staffed hundreds of hospitals across the United States, employed tens of thousands of physicians, and operated across virtually every major metro area. A 2023 report by the American Antitrust Institute found that in some markets, a single private equity-owned staffing firm controlled more than 30 percent of market share in emergency medicine staffing [1].
The revenue engine was out-of-network billing. When a patient with insurance visits an in-network emergency room, they typically expect their insurer to cover the bulk of the cost. What millions of patients discovered, sometimes months after the visit, when the bills arrived, was that while the hospital was in their insurance network, the physicians treating them worked for a separate company that was out-of-network. That company could bill at dramatically higher rates. Patients were on the hook for the difference, often without any advance notice.
A 2019 Yale study published by the National Bureau of Economic Research found that 39 percent of emergency department visits for one large insurer involved out-of-network physicians at in-network hospitals [1]. Envision and EmCare, its ER staffing subsidiary, featured prominently in the research. As one healthcare economist told MedPage Today after Envision’s bankruptcy: out-of-network billing was the company’s “secret sauce.” It was the source of the margin that justified a $9.9 billion acquisition price [1] and $8 billion in debt.
Doctor Patient Unity, a lobbying front group funded by KKR-owned Envision and Blackstone-owned TeamHealth, spent more than $57 million on advertising and lobbying between 2019 and 2020 [5] to block the federal No Surprises Act, which would eliminate most out-of-network emergency billing. The campaign ran ads claiming that patients needed to be “protected” from insurance companies, framing the bill as an insurer power grab rather than a patient protection measure. Senator Jeanne Shaheen and investigative journalists traced the funding: it came from private equity. When Congress passed the No Surprises Act in December 2020, with it taking effect in January 2022, the law eliminated the surprise-billing business model. For Envision, which had borrowed $8 billion on the assumption [1] that this revenue would continue indefinitely, the consequences were fatal.
The Network
KKR’s acquisition of Envision closed in October 2018. The transaction made Envision private and loaded it with approximately $8 billion in debt [1], the standard private equity structure of using borrowed money to finance the acquisition itself, with the acquired company responsible for servicing the debt. KKR’s strategy was to grow Envision’s hospital contract base, cut administrative costs, and exit through a secondary sale or IPO before the debt became unmanageable.
Blackstone Group acquired TeamHealth in 2017 in a transaction valued at approximately $6.1 billion [1]. TeamHealth, Envision’s primary competitor, operated similarly, staffing hospital emergency departments, anesthesiology suites, and intensive care units with physicians employed by the firm.
The third major player, SCP Health, private equity firm Onex backed the chain, formerly Schumacher Clinical Partners. Together, these three firms had achieved what amounted to an oligopoly in outsourced emergency medicine: they staffed a substantial share of American emergency departments, operated without meaningful federal oversight of their ownership structures, and generated revenue primarily through billing practices that patients didn’t understand and couldn’t anticipate.
The physicians inside these systems described a different experience than the efficiency narrative suggested. Emergency physicians working for Envision and TeamHealth reported that the firms evaluated them on metrics tied to billing volume and patient throughput rather than clinical outcomes [1]. Management reviewed clinical decisions, how long to observe a patient, when to order additional tests, whether to admit, against financial benchmarks [1]. Physicians who raised quality concerns or pushed back against discharge pressure described retaliation. The American Academy of Emergency Medicine Physician Group filed a lawsuit against Envision in California on December 20, 2021 [1], alleging that the company’s structure, a lay entity controlled by a private equity firm, violated the state’s prohibition on the corporate practice of medicine, which bars non-physician entities from making clinical decisions.
Joel Freedman, CEO of American Academic Health System, acquired Hahnemann University Hospital in Philadelphia in January 2018 for approximately $170 million [6], a 171-year-old teaching hospital and safety-net facility serving the city’s most vulnerable residents. The buyer structured the acquisition around the real estate. In June 2019, Freedman announced the hospital would close. It shut its doors in September 2019. Hahnemann had been the primary trauma center and safety-net hospital for downtown Philadelphia. Freedman sought to convert the building to luxury apartments and sell the medical residency slots, which are publicly funded, for profit. A bankruptcy judge later blocked the sale of residency positions. The hospital closure displaced hundreds of physicians, terminated the training programs of hundreds of medical residents, and eliminated emergency care access for tens of thousands of patients in one of the country’s poorest urban neighborhoods.
A 2023 JAMA study found a link between private equity acquisitions and reduced emergency department staffing, increased patient mortality, and higher hospital-acquired infection rates.
What Was Buried
The evidence that private equity ownership harmed patient outcomes was accumulating in academic journals years before the policy response caught up.
A landmark study published in JAMA in December 2023, authored by Sneha Kannan and colleagues, examined 51 private equity-owned hospitals and found a 25 percent increase in hospital-acquired conditions [3], including infections, falls, and medication errors, following private equity acquisition, compared to matched non-PE hospitals. The National Institutes of Health published a summary of the findings in January 2024. The mechanism, the researchers noted, was consistent with what physicians inside these systems had described: cost-cutting in nursing and support staff, pressure to discharge patients earlier, reduced investment in infection control infrastructure.
Harvard Medical School researchers published related findings in September 2025 [4], examining emergency department deaths specifically after hospital acquisition by private equity firms. The study found that emergency department deaths rose more than 13 percent following PE acquisition [4]. A Harvard publication summarizing the work was blunt: “staffing and salary cuts likely explain the increase in patient deaths in the emergency departments of hospitals acquired by private equity firms.” The New England Journal of Medicine published research linking PE hospital acquisitions to increased deaths following emergency surgeries as well.
The American College of Emergency Physicians, in a September 2025 analysis, found a link between private equity acquisitions and reduced emergency department and intensive care unit staffing expenditures. In emergency medicine, reduced staffing is not an abstract efficiency gain. It means longer waits for sicker patients, more errors at the margin, and worse outcomes for people who arrive in crisis.
These findings, 25 percent more hospital-acquired infections [3], 13 percent more ER deaths [4], documented staffing reductions, were not available when KKR acquired Envision for $9.9 billion in 2018 [1]. They were accumulating in the research literature while the private equity model was at its peak. The Senate Homeland Security and Governmental Affairs Committee published an investigation in April 2024 examining the KKR-Envision relationship specifically, documenting how financial decisions made in the service of debt service affected the availability and quality of emergency care. The Senate committee report came five years after the acquisition. By then, Envision was in bankruptcy.
A ScienceDirect analysis published in 2025 found that between 2014 and 2022, private equity-backed healthcare companies paid more than $500 million to settle at least 34 lawsuits filed under the False Claims Act [1], federal fraud claims involving overbilling Medicare and Medicaid. The settlements were primarily in billing fraud, the downstream consequence of financial pressure applied to billing departments by private equity ownership.
The Stakes Now
Envision’s bankruptcy did not end private equity’s presence in American emergency medicine. TeamHealth, still owned by Blackstone, continues to operate. SCP Health continues to staff hospital EDs across the country. According to an American Progress analysis published in October 2025, private equity firms have continued aggressively acquiring health systems, hospitals, physician practices, and ancillary services throughout the post-Envision period. The bankruptcy was a financial event, not a regulatory one. No law was broken. No executive was charged. No structural reform was mandated.
The Health Over Wealth Act, introduced in July 2024 by Representative Pramila Jayapal and Senator Ed Markey, would establish guardrails for private equity investment in healthcare, including restrictions on the debt-loading and financial engineering that made the Envision model possible. As of early 2026, it has not passed. In February 2026, Senator Elizabeth Warren co-introduced legislation targeting private equity abuse in healthcare following the bankruptcy of Genesis Healthcare, a nursing home chain. The legislation aimed to ensure that private equity firms cannot use bankruptcy to escape liability to patients and their families. It has not passed either.
The structural conditions that enabled the Envision model remain in place. Hospitals still outsource physician staffing. The transparency in healthcare billing that would let patients know before treatment whether their physician is in-network remains limited. Federal restrictions on private equity ownership of medical practices exist in some states and not others. The No Surprises Act eliminated the specific billing arbitrage that made Envision profitable, but private equity has already identified new revenue vectors in healthcare: home health, behavioral health, specialty pharmacy, and nursing facilities.
The Senate HSGAC report on Envision, published in April 2024 as part of a broader investigation titled “Profits over Patients [1],” documented the pattern in detail: acquisition for financial engineering purposes, debt-loading that prioritizes debt service over patient care investment, staffing reductions to meet margin targets, and billing practices that shift costs to patients and government programs. The report’s title was accurate. What it did not answer was how to stop the next iteration.
The agency that approves the drugs prescribed in those emergency rooms operates with the same revolving-door pattern: nine of the last ten FDA commissioners now work for the companies they regulated.
The One Thing That Matters
The private equity model in emergency medicine generated profit precisely because patients cannot avoid the emergency room. You do not choose to have a heart attack. You do not schedule your emergency. The EMTALA guarantee, that any hospital with an emergency department must treat you, was designed to protect patients. Private equity turned it into a captive revenue guarantee. KKR loaded Envision with $8 billion in debt on the assumption [1] that sick people would keep showing up and that the billing would keep working. The patients kept showing up. The billing eventually didn’t. What the Harvard researchers found in the years between, the 13 percent rise in emergency room deaths [4], the 25 percent rise in hospital-acquired [3] infections, those are the human costs of treating emergency medicine as a financial instrument. The numbers in the bankruptcy filings are large and abstract. The number that matters is how many people died in emergency rooms that had been stripped of staff to service debt that was never theirs.
Sources: Pestakeholder.org, “KKR and Blackstone-owned Firms Have Spent Millions to Oppose a Ban on Surprise Medical Billing” (September 2019); MedPage Today, “No Surprises Act Ruined ‘Secret Sauce’ of Envision” (June 2023); Reuters, “Bankrupt Envision Healthcare approved to split in two, cut debt” (October 2023); JAMA, Kannan et al., “Changes in Hospital Adverse Events and Patient Outcomes Associated with Private Equity Acquisition” (December 2023); NIH Research Matters, “Infections and falls increased in private equity-owned hospitals” (January 2024); Harvard Medical School news, “Deaths Rose in Emergency Rooms After Hospitals Were Acquired by Private Equity Firms” (September 2025); AAEM Envision lawsuit filing (December 2021); Senate HSGAC KKR-Envision investigation (April 2024); Senate HSGAC “Profits over Patients” Report (November 2024); American Progress, “5 Consequences of Private Equity’s Expansion in Health Care Services” (October 2025); Senator Warren/Goodlander PE legislation (February 2026); Health Over Wealth Act, Jayapal/Markey (July 2024); ScienceDirect, “Private equity expansion and impacts in United States healthcare” (2025); The New Yorker, “The Death of Hahnemann Hospital” (May 2021).
How we know
Every factual claim above traces to one of the entries below. Paywalled sources are marked. Where a source might disappear, the archive link points to a snapshot.
- 01
- 02
- 03
- 04
- 05
-
06
The Death of Hahnemann Hospital paywall
This piece relies on the Senate HSGAC investigation into KKR-Envision (2024) and the subsequent 'Profits over Patients' report (November 2024); Reuters' coverage of the Envision bankruptcy filing; the JAMA Kannan et al. study on adverse events at PE-acquired hospitals (December 2023); and the Harvard Medical School research on ER mortality (2025). Lobbying-spending figures cite OpenSecrets disclosures. The Hahnemann Hospital details come from The New Yorker's 2021 reporting.